
Guideline Updates
- International consensus statement on quality standards for managing children/adolescents with bronchiectasis from the ERS CRC Child-BEAR-Net
- WAO-ARIA consensus on chronic cough – Part III: Management strategies in primary and cough-specialty care
- Canadian Thoracic Society 2021 Guideline update: Diagnosis and management of asthma in preschoolers, children and adults
- NICE 2021 guidelines on Cough (acute): Antimicrobial prescribing
- ERS guidelines on the diagnosis and treatment of chronic cough in adults and children
International consensus statement on quality standards for managing children/adolescents with bronchiectasis from the ERS CRC Child-BEAR-Net

Eur Respir J. 2022;59(6):2200264
Bronchiectasis is a clinical syndrome encompassing recurrent or persistent wet/productive cough with abnormal bronchial dilatation as seen in chest computed tomography (CT) images.
While the quality of care for people with bronchiectasis is inequitable, the ELF-PAG for the European Respiratory Society (ERS) clinical practice guideline for managing bronchiectasis in children and adolescents expressed the urgent need for standardised quality care.
What exists and what is needed?
- Quality standard statement based on the Birtish Thoracic Society (BTS) guidelines are available for the management of bronchiectasis in adults in the UK and other European countries.
- However, such documents are currently not available for bronchiectasis in children.
- The Child-BEAR-Net (Children’s Bronchiectasis Education, Advocacy and Research Network) aimed to fill this gap.
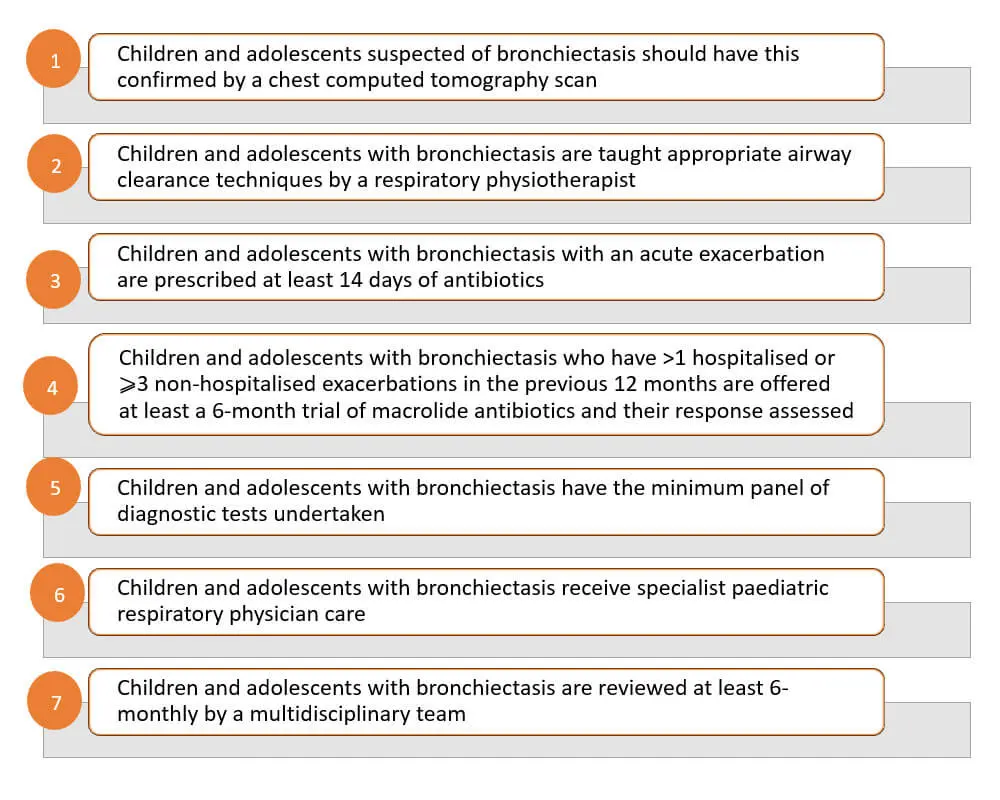
Quality standard statements for clinically significant bronchiectasis in children and adolescents
The CRC panel and European Lung Foundation-established parent advisory group (ELF-PAG) unanimously and independently endorsed these seven quality standard statements.
References:
Chang AB, Boyd J, Bush A, et al. International consensus statement on quality standards for managing children/adolescents with bronchiectasis from the ERS CRC Child-BEAR-Net. Eur Respir J. 2022;59(6):2200264.
WAO-ARIA consensus on chronic cough – Part III: Management strategies in primary and cough-specialty care

- This third part of the WAO/ARIA consensus on chronic cough suggests a management algorithm of chronic cough in an integrated care pathway approach.
Empirical treatment in primary care
Oral antihistamine therapy in patients with rhinitis and cough is not recommended because of their low efficacy in reducing cough.
Upper airway
- 4-week therapy with intranasal corticosteroids in allergic rhinitis (AR) patients with upper airway disease-related cough.
- Therapy can be tapered in patients showing improvement.
- Patients with partial or no improvement can be referred to cough specialty care.
Lower airway
- No clear role of pharmacotherapy.
- An initial 2-week empirical trial of short-acting bronchodilator supplemented with inhaled corticosteroids (ICS) may be warranted in chronic cough patients.
- If patient cannot tolerate ICS, a short course of oral corticosteroids can be prescribed.
Gastrointestinal (GI) tract
- Behavioral changes (e.g., weight reduction and dietary changes) are recommended in patients with GERD irrespective of concomitant cough.
- An initial 4–12-week empirical and diagnostic trial of proton pump inhibitors (PPIs) can improve a proportion of patients (confirming diagnosis of GERD-related cough).
- PPI therapy can be tapered to the lowest dose for control of cough.
- Patient should be referred to a GI specialist for further investigation of underlying gastrointestinal disorders or in case of PPI failure/dependency.
Guidelines and expert consensus in cough pharmacotherapy
Upper airways
- The role of pharmacotherapy is inconclusive.
Lower airways
- Clinical profile reminiscent of asthma: Several drugs can be offered; studies suggest improvement cough scores with ICS, leukotriene receptor antagonists (LTRAs), inhaled beta2-agonists and muscarinic receptor antagonists, and extent theophylline and mast cell stabilizers (lesser extent).
- Suspected cough-variant asthma (CVA): Recent guidelines recommend ICS as first line treatment. Careful interpretation of the benefit of ICS in nonspecific cough is required.
- Suspected non-asthmatic eosinophilic bronchitis (NAEB): A therapeutic/diagnostic trial of ICS followed by LTRAs (if stepping up ICS fails to improve cough).
- Chronic obstructive pulmonary disease (COPD): An empirical trial of bronchodilator therapy is often justified but requires more efficacy data.
Digestive tract
- Early (within 2 weeks) cough improvement on PPIs, followed by 4–12 weeks of maintenance therapy before tapering medications. Night-time magnesium and melatonin supplementation is recommended for partial responders.
- Supplementing PPI therapy with prokinetics can enhance gut motility and improve gastroesophageal reflux disease (GERD)-related cough.
- Adding H2-blockers for 2–4 weeks can reduce nocturnal acid breakthrough in difficult-to-treat cases of GERD (role in cough has not been investigated).
- Neuromodulators (e.g., baclofen) in combination with PPI can benefit patients with loose lower esophageal sphincter or high reflux symptom index (RSI) scores.
Reference: Rouadi PW, Idriss SA, Bousquet J, et al. WAO-ARIA consensus on chronic cough – Part III: Management strategies in primary and cough-specialty care. Updates inCOVID-19. World Allergy Organ J. 2022;15(5):100649.
Canadian Thoracic Society 2021 Guideline update: Diagnosis and management of asthma in preschoolers, children and adults

An overview of pharmacologic treatment recommendations
- Consider the type of inhaler device that a patient prefers to use and can use properly before prescribing asthma medication
- All asthmatics should have access to a releiver to treat acute symptoms
- In Canada, short-acting beta-agonists (SABAs; salbutamol, terbutaline), and a combination inhaler (bud/form) are approved for this indication.As needed bud/form is approved for use as a reliever in adults and children ≥12 years of age (in Canada).
- Bud/form should not be used as a reliever when controller medications other than maintenance bud/form are used.
- SABAs should only be used for symptom relief and should not be regularly used “to open the airways” before daily controller therapy administration.
- The safest and minimum effective inhaled corticosteroids (ICS) dose that achieves the goals of current control and eliminates exacerbations, should be prescribed to minimize side effects (all groups).
- In poorly controlled asthma cases , potential should be assessed and corrected prior to or in conjunction with escalation of pharmacologic therapy.
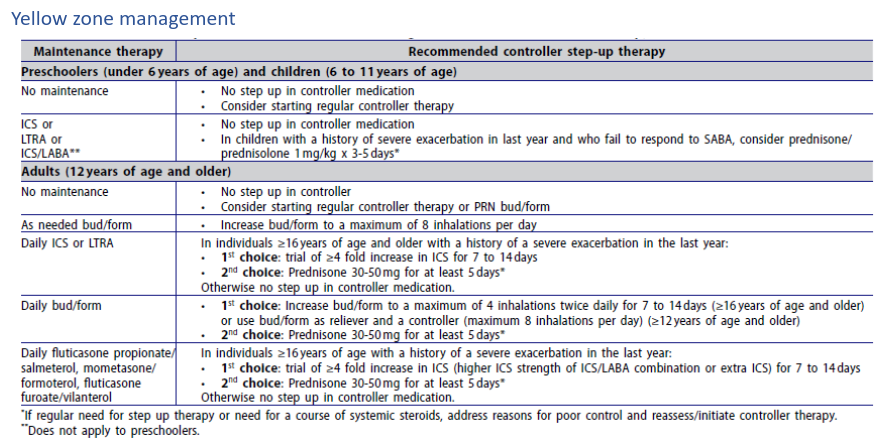
Patients not on controller therapy
- Well controlled on SABA or no medication with a lower risk for exacerbations : Continue PRN SABA or be switched to either daily ICS + PRN SABA (all ages) or PRN bud/form (≥12 years of age
- Well-controlled on PRN SABA or no medication with higher risk for exacerbations : Should not be on PRN SABA; switch to daily ICS + PRN SABA (all ages) or PRN bud/form (≥ 12 years of age)
- Not controlled on PRN SABA or no medication : Daily ICS + PRN SABA
- Second line to daily ICS : Leukotriene receptor antagonists (LTRAs) in patients of all ages
Patients not achieving control on low dose ICS
Children not achieving asthma control despite adherence to low dose ICS should be increased to medium dose ICS.
Reference: Yang CL, Hicks EA, Mitchell PA, et al. Canadian Thoracic Society 2021 Guideline update: Diagnosis and management of asthma in preschoolers, children and adults. Canadian J Resp Crit Care Sleep Med. 2021;5(6): 348–361.
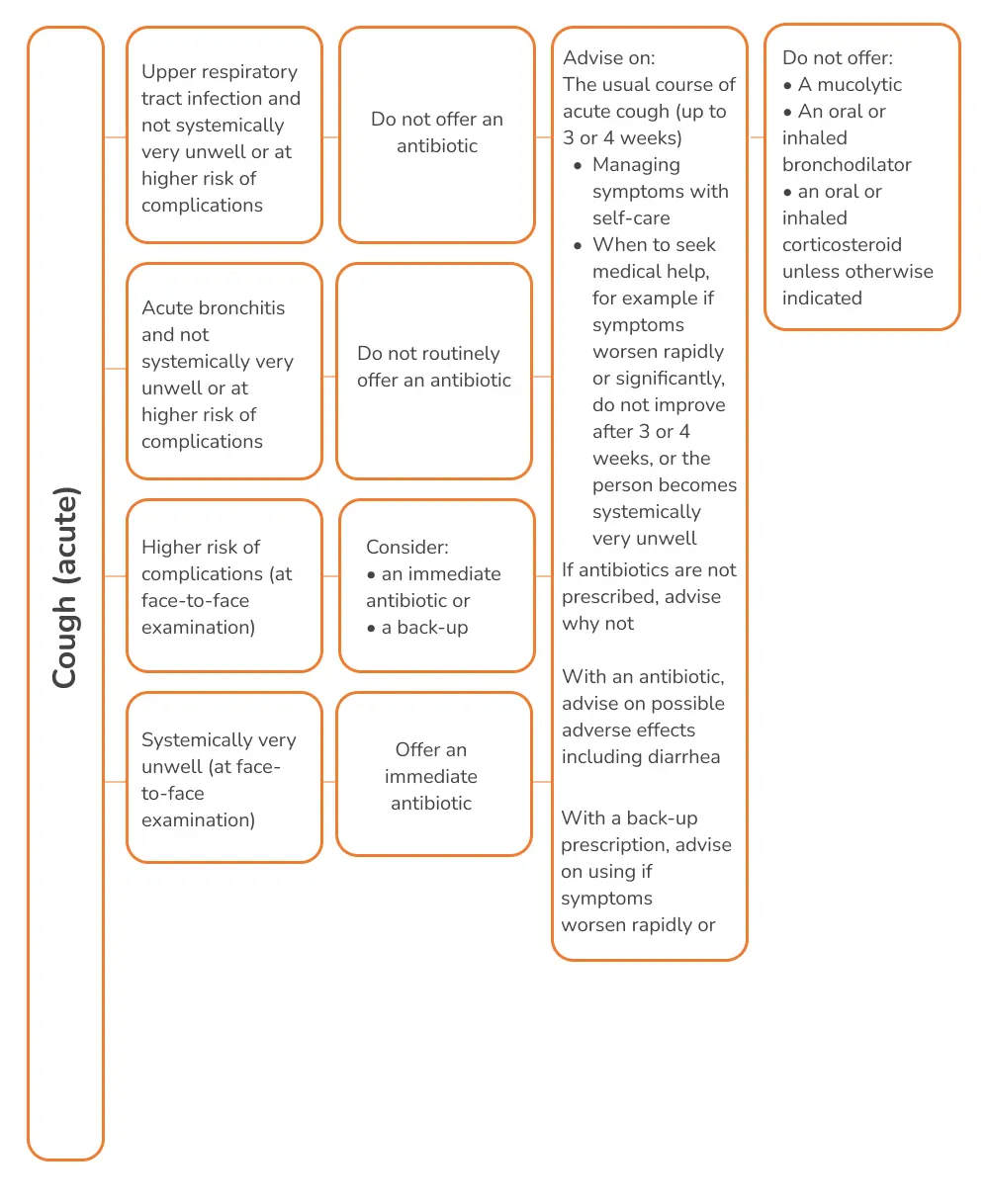
NICE 2021 guidelines on Cough (acute): Antimicrobial prescribing
According to the committee discussion, acute cough, either associated with an upper respiratory tract infection or acute bronchitis, is usually a self-limiting infection. It is often a viral infection, and antibiotics are not usually needed.
Recommendations on when antibiotics are not required, are required immediately, or as back-up
Recommendations on the choice of antibiotic
- A narrow-spectrum antibiotic should generally be first choice, when an antibiotic is needed.
- Where an antibiotic is appropriate, doxycycline at usual dose is recommended, as the first-choice antibiotic for adults with acute cough (including acute bronchitis), in non-pregnant adults, and in young people >12 years.
- Amoxicillin, clarithromycin or erythromycin should be offered as alternative first choices; for children and young people, amoxicillin is recommended as the first-choice antibiotic in such scenario.
Recommendations on antibiotic course length
- The shortest course that is likely to be effective should be prescribed. A 5-day course for all the recommended antibiotics is sufficient to treat acute cough.
Reference: NICE guideline. Available at www.nice.org.uk/guidance/ng120
ERS guidelines on the diagnosis and treatment of chronic cough in adults and children
According to the guideline panel, it is preferable to undertake sequential therapeutic trials of each agent in turn and if no responses are observed therapy should be stopped. The length of the trial depends on the pharmacology.
Pharmacological control
Recommendations for using anti-asthmatics
- A short-term ICS trial (2–4 weeks) in adult patients with chronic cough
- A short-term ICS trial in children with chronic dry cough (2–4 weeks)
- A short-term antileukotriene trial (2–4 weeks) in adults with chronic cough, particularly in those with asthmatic cough
- A short-term trial (2–4 weeks) of ICS and long-acting bronchodilator combination in adults with chronic cough and fixed airflow obstruction
Recommendations for using anti-acids
- It is recommended that clinicians do not routinely use anti-acid drugs in adult patients with chronic cough
Recommendations for using drugs with promotility activity
- There is currently insufficient evidence to recommend the routine use of macrolide therapy in chronic cough. A 1-month trial of macrolides can be considered in the cough of chronic bronchitis refractory to other therapy, considering local guidelines on antimicrobial stewardship.
Recommendations for using neuromodulatory agents
- A trial of low-dose morphine (5–10 mg twice daily) in adult patients with chronic refractory cough we suggest a trial of gabapentin or pregabalin in adult patients with chronic refractory cough.
Nonpharmacological control
- A trial of cough control therapy in adult patients with chronic cough is recommended.
Antibiotics for chronic wet cough in children
- A trial of antibiotics is suggested in children with chronic wet cough with normal chest radiographs, normal spirometry and no warning signs.
Reference: Morice AH, Millqvist E, Bieksiene K, et al. ERS guidelines on the diagnosis and treatment of chronic cough in adults and children. Eur Respir J. 2020;55(1):1901136.

An initiative by Glenmark to educate about everything related to Cough and spread awareness about cough related health conditions.
Quick Links
Contacts
- GLENMARK PHARMACEUTICALS LIMITED Glenmark Corporate Enclave, BD Sawant Marg, Chakala, Off WE Highway, Andheri (E), Mumbai 400099
- Terms & Condition
- Privacy Policy
- Sitemap
- Disclaimer
- Coughology © 2024 All Right Reserved